
Background
- Diabetic foot problems are the most common cause of non-traumatic limb amputation
- Life expectancy can be reduced by up to 15 years for people with diabetes
- 15% of people with diabetes will have a foot ulcer at some point in their lives
History
- Previous ulceration
- Previous amputation
- Symptoms of neuropathy (numbness, tingling, burning)
- Symptoms of vascular disease
- Onset of presenting problem
- Diabetes control and medication
Remove the patient’s shoes, socks and dressings and examine their feet
Both feet should be examined for
- Dorsalis pedis pulse
- Posterior tibial pulse
- Temperature (cool-ischaemic) warm/hot (?infection)
- Peripheral sensory neuropathy
Look for
- Discolouration in foot, Ulceration, Blisters, Necrosis
- Callus with signs of underlying extravasation, capillary leakage
- Red areas, Swelling, Infection/Cellulitis, ↑ body temperature, Flu-like symptoms
- Poor glycaemic control
- Pain in foot or leg even in presence of neuropathy
Remove the patient’s shoes, socks, bandages and dressings and examine their feet.
Specialist referral

If the following are present, obtain urgent advice from an appropriate specialist:
- Charcot’s arthropathy (which should be considered if deformity, redness or warmth are present.)
- Systemic sepsis
- Deep seated infection
- Limb ischaemia
If osteomyelitis is suspected
- If initial X-ray unconvincing, use MRI
- If MRI is contraindicated admit for white blood cell (WBC) scanning
Neuropathic ulcer


- May have heavy callus build up
- Found on weight bearing areas of foot
- Punched out appearance
- Usually pedal pulses can be palpated
- Can be deceptive as ulcer may penetrate to bone
- May present with localised/spreading infection
- Usually painless
Treatment
- Non adherent dressing to wound (± larger temporary shoe)
- Broad-spectrum antibiotic in presence of localised infection
- Urgent admission for bed rest and i/v antibiotics if spreading cellulitis
- X Ray for osteomyelitis
- Refer to podiatry for callus reduction, wound/footwear assessment and multi-professional management
Neuro-ischaemic ulceration

Clinical signs
- Minimal callus build-up
- Ulcers often located on borders of foot where there may be pressure from footwear
- Pedal pulses non-palpable
- Often painful
- May be infected or appear necrotic/gangrenous
Treatment
- As above
- May require urgent vascular referral
Charcot's Neuro-arthropathy
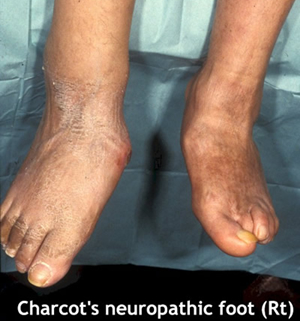
Presenting symptoms
- Hot swollen foot, ± history of injury
- Peripheral sensory neuropathy
- Bounding foot pulses
- Differential diagnosis to eliminate osteomyelitis
- Early radiological signs absent
- Gold standard to Dx is technetium bone scan
Treatment
- Treat as though diagnosis confirmed while awaiting definitive diagnosis
- Non weight-bearing cast changed at weekly intervals until foot no longer hot and x-ray indicates resolution
- Too rapid mobilisation can be disastrous and lead to further bony changes
- It is essential to differentiate between Charcot’s and cellulitic foot
Links
- Podiatrist CUH on site in OPD (next to fracture clinic) - Tuesday, Thursday, Friday
- NICE Guideline 2011 - Diabetic foot problems - inpatient management