History
Hyperabduction of the thumb with pain and swelling, especially around the MCP joint. Note occupation & previous injury.
Examination
- Check the stability of the MCP joint
- Instability with or without a Stener lesion will determine your following treatment plan (see Fig 3)
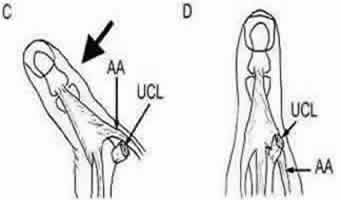
- Stener lesions occur when joint hyperabduction leads to the adductor aponeurosis becoming interposed between the ends of the UCL (see Fig 1). As the ends of the UCL are unopposed healing will not occur and the joint will remain unstable
- Patient will have pain around the MCP joint, especially over the ulnar aspect
- Localised swelling may be detected on the ulnar aspect of the MCP joint, which might indicate a Stener lesion (i.e. the swelling is caused by the displaced ligament)
- Examine the rest of the thumb for other possible injuries (tendon injuries; instability of other joints; nerve and vascular damage)
Investigations

- X-ray before stressing the joint, to ascertain if a fracture is present or if there is volar subluxation at the MCP joint (suggesting UCL injury)
- If a fracture is present or there is volar subluxation discuss with the on call team, especially if the fragment is displaced or involves a significant amount of joint space
- If no fracture and not uncomfortable , gently stress joint for stability
- ± ring or median and radial nerve block, local infiltration
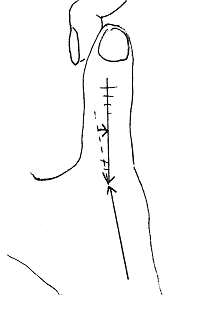
- To stress the joint: immobilise the MC with your thumb and index finger of one hand, and use your other hand to gently hyperabduct the thumb (Fig 2)
- Stress in full extension and 30° of flexion
- Compare with the non-injured thumb
- Angulation over 35° or lack of firm end point, or 15° > the non-injured thumb indicates instability (in both extension and 30° flexion)
Management
When available, functional splintage should be used in this group of patients rather than plaster casts.[BestBets]. Results similar with the us eof a functilnal slint, PoP or surgery are involved.