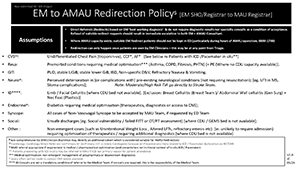
Do not require diagnostic results nor specialty consults as a condition of acceptance
Refusal of suitable redirect requests should result in immediate escalation to both EM & AMAU Consultant
Where AMAU capacity exists, suitable EM Redirect patients should not be kept in ED (particularly during hours of AMAU operation, 0800 1700)
Redirection can only happen once patients are seen by EM Clinicians - this can be any point from triage
Examples
CVS $$: Undifferentiated Chest Pain (troponin -ve ), CCF*, AF* [See below re Patients with ICD /Pacemaker in-situ]
Resp: Premorbid conditions requiring medical optimisation*** (Asthma, COPD, Fibrosis, PHTN) [+ PE (Where no CDU capacity available
GIT: PUD, stable UGIB , stable lower GIB , IBD, Non specific D& Refractory Nausea & Vomiting
Neuro^: Perceived deterioration in (or complications with) pre existing neurological conditions (not requiring resuscitation); e.g. . UTI in MS, Stoma complications]; Note: Moderate/High Risk TIA go directly to Stroke Team
ID****: Limb / Facial Cellulitis [where CDU bed not available]. [Exclusion: Breast Cellulitis (Breast Team )/ Abdominal Wall cellulitis (Gen Surg ) + Nec Fasc (Plastics)]
Endocrine^: Diabetics requiring medical optimisation (therapeutics, diagnostics or access to CNS)
Syncope: All cases of Non Vasovagal Syncope to be accepted by MAU Team, if requested by EM Team
Social: Unsafe discharges ( e.g. Social vulnerability / failed FITT or OT/PT assessment) [where CDU / GEMS bed is not available]
Other: Non emergent cases (such as Unintentional Weight Loss , Altered LFTs, refractory emesis etc ) i.e. . unlikely to require admission) but requiring optimisation of therapeutics / requiring additional diagnostics [where CDU bed is not available]
Key
$ non comprehensive list
$$ Cardiology : Cardiology Direct Referrals: (a) Primary AF (b) Primary CCF (c) Likely Cardiogenic Syncope (d) Presentations likely related to ICD / Pacemaker dysfunction (e) NSTEMI
* MAU referral appropriate if requirement is medical / pharmaceutical optimisation (and presentation not in clinical context of in-situ ICD / Pacemaker)
** Patients presenting with ICD in-situ may be referred to MAU if ICD is not the primary reason for patient attendance
*** Medical optimisation: non emergent management of polypharmacy or downstream diagnostics
^ every effort will be made to contact CNS where available
**** ID Consults are not a mandatory condition of referral