Definition
Acute otitis media is the presence of a middle ear effusion accompanied by rapid onset of one of otalgia, otorrhoea, irritability in an infant or toddler, or fever.
Acute otitis media (AOM) is a common problem in early childhood with 2/3 of children experiencing at least one episode by age 3, and 90% have at least one episode by school entry. Peak age prevalence is 6-18 months
Aetiology
- Viral (25%)
- Strep. pneumoniae (35%)
- H. influenzae (25%)
- Moraxella catarrhalis (15%)
Assessment
- Note: A child with otitis media can also have serious bacterial infection such as septicaemia or meningitis
- If systemically unwell, consider coexistent causes of sepsis - do not accept otitis media as the sole diagnosis in a sick febrile young child without elimination of a more serious cause
History
- Fever, ear pain (irritability) ± anorexia, vomiting, lethargy
Examination
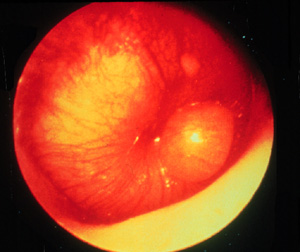
- The usual middle ear landmarks (handle of malleus, incus, light reflex) are not well seen
- The tympanic membrane (TM) is dull and opaque, and may be bulging
- The TM colour varies but is characteristically yellow-grey
- On pneumatic otoscopy TM mobility is reduced
- There may be associated signs of URTI, such as coryza, red tonsillopharynx, cough etc
- The features suggest the infection is viral
- Many febrile or crying children have red TMs (just as they have red cheeks). A red TM alone is not acute otitis media.
- It is not usually necessary to remove wax from the ear canals of febrile children
Pitfalls
Otitis media can coexist with other diseases such as meningitis. Ask yourself ...does the diagnosis fit the rest of the presentation?
- Ear pain can be caused by other pathology e.g. URTI causing eustachian tube dysfunction, foreign body, otitis externa
- Otalgia may also be referred from other facial, oral and cervical structures
- In very young children otitis media may be secondary to bacteraemia from other sources
- A middle ear effusion can persist for a variable length of time following an episode of AOM
- Not all children with an ear effusion have AOM
Complications
- Perforation of the TM results in purulent otorrhoea, and relief of pain
- Febrile convulsions are commonly related to AOM
- Suppurative complications such as mastoiditis, suppurative labyrinthitis or intracranial infection (meningitis, extradural or subdural abscess, brain abscess) are uncommon
- Other potential complications include facial nerve palsy, lateral sinus thrombosis, and benign intracranial hypertension
Serous otitis media ("glue ear")
Serous middle ear effusion commonly persists for several weeks or even months following an episode of AOM. This may be recurrent, even in the absence of identifiable episodes of AOM, and often causes conductive hearing loss. The long-term effects on language, literacy and cognitive development are unclear. Parental smoking is an important avoidable risk factor. The use of dummies should be limited to settling, as prolonged use has been shown to be associated with otitis media.
Management AOM
- Most cases (80%) of AOM in children resolve spontaneously in 3 days
- Overall, antibiotics reduce the incidence of an extended course of acute otitis media at 3-7 days by 13%, with an NNT of 8 [Bandolier]
- The use of antibiotics does not reduce the incidence of complications, including hearing problems
- The modest benefit must be weighed against the potential harms related to antibiotic use, both for the individual patient (adverse effects) and at a population level (resistance pressure)
- It has been shown that not using antibiotics for otitis media is acceptable to parents if the reasons are explained clearly
- Pain is often the main symptom, so adequate analgesia is very important:
- Paracetamol (20-30 mg/kg for 2-3 doses/day) should be given if pain is significant
- Short-term use of topical 1% lignocaine drops applied to the TM may give relief
- Decongestants, antihistamines and corticosteroids have not been shown to be effective in AOM
- Pus from a ruptured tympanic membrane should be cultured
Reference / Links
- IAEM - AOM guideline
- Does This Child Have Otitis Media? Rothman R, Owens T, Simel D. JAMA 2003;290(12):1633-1640
- SIGN guidelines index
- Bandolier
- MM Rovers et al. Antibiotics for acute otitis media: a meta-analysis with individual patient data. Lancet 2006 368:1429-1435