Myeloma
Background
- B-cell lymphoid malignancy
- Clonal proliferation of plasma cells (synthesize abN Ig) in marrow
- Commonest primary malignant tumour of bone (1% of bone Tu)
- No specific risk factors
Clinical
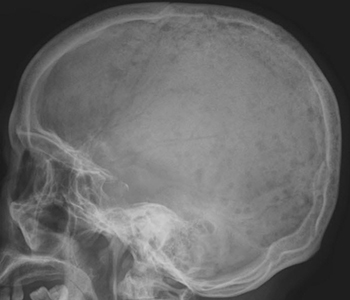
- May present as incidental finding (e.g. x-ray, ↑ESR, ↑Ca++) or very aggressive painful bony destruction
- Often background history of renal symptoms or vague constitutional symptoms (anaemia)
- Rarely recurrent infections : hypogammaglobulinaemia
Major criteria
- Monoclonal protein on electrophoresis or Bence Jones proteinuria >1 g/24 hr
- Bone marrow plasma cells at least > 10%
- Lytic bony lesions
Minor criteria
- Cytopenia (esp. ↓Hb or ↓Platelets)
- Renal failure and hypercalcaemia
- Hyperviscosity (SOB, confusion, chest pain)
Investigations
- MRI useful for vertebral lesions
- Chromosomal abnormalities may help with prognosis
- ESR may be normal (non-Ig producing myeloma)
Treatment
- Stage the condition (based on B marrow, proteinuria load on electrophoresis etc.)
- Confirm renal status, chromosomal abnormalities and Plasma Cell Labelling Index (PCLI)
- Aim to control disease and manage symptoms (beware electrolytes, ↑Ca++, renal fxn and cytopaenias)
- Aggressive appropriate analgesia as required
- Options include chemoRx, radioRxs, immunomodulation and marrow transplant
Content by Dr Íomhar O' Sullivan. Last review Dr ÍOS 12/04/23.