Background
Classified on serum level
- Mild = 5.5 - 6.0mmol/l
- Moderate 6.1 - 6.9mmol/l
- Severe >7 mmol/l
Can cause cardiac standstill and VF
Causes
- Acute renal failure
- K+ sparing diuretics
- ACE inhibitors
- Hyperglycaemia
- Rhabdomyolysis
- Adrenal insufficiency
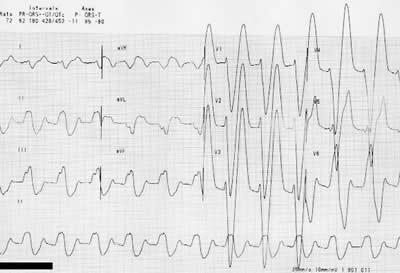
Small broad P or absent P waves
Wide QRS complex (K+ 7-8 mmol/l)
Sinusoidal QRST (K+ 8 - 9 mmol/l)
AV dissociation or VT / VF (K+ >9 mmol/l)
Management
Calcium gluconate
- 30ml of 10% Ca++ gluconate over 10 minutes
- Indicated when ECG changes present
- Antagonises cardiac excitability
- Does not affect plasma potassium level
- Duration of protection - minutes. Repeat as necessary
- Slower (over 30 min) infusion in patients on digoxin
Insulin with glucose
- Stimulates Na+ - K+ ATP pump and so intracellular uptake of K+
- Dose = 10iu insulin in 50ml of 50% dextrose given as bolus
- In children a glucose load of 0.5 g/kg/hr (2.5ml/kg/hr) should be given. If blood glucose rises above 10 mmol/l then insulin should be added at 0.05u/kg/hr
- Onset of action 15 min, lasts about 1 hour
Salbutamol
- Binds B2, stimulates CAMP, which stimulates Na+-K+ ATP pump
- Give 0.5mg (4 µg/kg in children) slow IV
- or
- 10mg nebulised Salbutamol (in children 2.5 mg if < 25kg, 5 mg if > 25 kg)
- Avoid IV admin. in patients with ischaemic heart disease
Sodium bicarbonate
- No effect on plasma level for 60 min
- No studies demonstrate clear benefit
- May be considered in severe acidosis
Sodium polystyrene sulphonate
- Resin binds K+ in the intestine
- 50 grams polystyrene in 100-200ml 30% sorbitol or 10% glucose
- Given PR and left for at least 60 min
Haemodialysis
- Definitive hypokalaemic measure
- Rapid fall in plasma level in first hour
- Especially where hyperkalaemic arrest or other medications have failed
Links
- Emergency Medicine Journal
- CUH Intranet only Pharmacy Guideline on Mx ↑K+ solution dilutions