Background
Prior to Prescribing of Unfractionated Heparin (UFH) for Therapeutic Anticoagulation
Review baseline APTT ratio, coagulation screen, FBC, U&Es and LFTs before starting UFH. Refer to Haematology Team:
- If baseline INR >1.5 and the patient is not on warfarin
- If patient has thrombocytopenia (e.g. platelets < 75 x 109/ L)
Target APTT Ratio
- The standard therapeutic range for UFH in CUH is an APTT ratio 2.0–2.5
- To use a target range other than APTT ratio of 2.0–2.5 a different dose adjustment table must be prescribed
Step 1: Loading Dose: See Step 1 for guidance and examples of when a loading dose may not be indicated.
Step 2: Maintenance Dose: Maintenance infusion should be started immediately after loading dose (if indicated). See Step 2 for guidance.
Step 3: Monitoring of APTT Ratio and Platelets
- Check APTT ratio 6 hours after starting UFH maintenance infusion, then adjust rate to achieve an APTT ratio 2.0–2.5 using the dose adjustment table (See table Step 3). Maintain the changed rate until next APTT ratio
- Check APTT ratio approximately 6 hours after each dose change. If APTT ratio is very high more frequent measurements are advised
- Exercise caution with renal/ hepatic patients as patients will be at a higher risk of bleeding
- Monitor patients for signs of Heparin Induced Thrombocytopenia (HIT) e.g.50% reduction count of platelets, thrombosis or skin necrosis. Refer to Haematology Team
Step 1 (loading/"bolus")
| Baseline APPTT ratio |
Administer IV loading dose over 5 minutes as a single dose, then refer to Step 2 for UFH maintenance infusion rate (ml/hour) |
|
|---|---|---|
| units | ml (1000 units/ ml) | |
| < 1.5 | 5000 units | 5 ml |
| 1.6 - 1.9 | 2500 units | 2.5 ml |
| ≥ 2.0 | Heparin is contraindicated. Contact Haematology team | |

For patients with a high risk of bleeding, a loading dose may not be required e.g.
- patients that received heparin in the previous 6 hours
- post stoke
- elderly >70 yrs
- Cr clearance < 30ml/min
- Low body weight
A revised APTT target ratio may be required if there is a high risk of bleeding. Please contact the Haematology team.
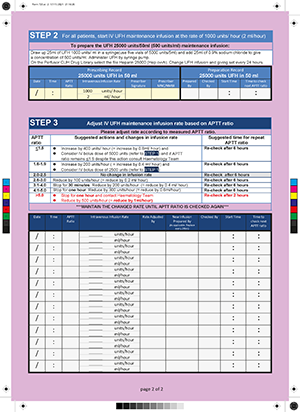
Step 2 (infusion)
| Draw up 25ml of UFH 1000 units/ ml in a syringe(use five vials of 5000 units/5ml) and add 25ml of 0.9% sodium chloride to give a concentration of 500 units/ml. Administer UFH by syringe pump. On the Perfusor CUH Drug Library select the file Heparin 25000 (Hep cvvh). Change UFH infusion and giving set every 24 hours. | ||||||||||
| Prescribing Record 25000 units UFH in 50 ml |
Preparation Record 25000 units UFH in 50ml |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Date | Time | APTT ratio |
IV infusion rate | Prescriber signature |
Prescriber MCN/NMBI |
Prepared by |
Checked by |
Start time |
Time to check APTT |
|
| 1000 | units/hr | |||||||||
| 2 | ml/hr | |||||||||
Step 3 (monitor and adjust)
Adjust IV UFH maintenance infusion rate based on APTT ratio
| APTT ratio |
Suggested actions and changes in infusion rate | Time to check APTT ratio |
|---|---|---|
| ≤1.5 | ↑ by 400 units/hr (= ↑ by 0.8ml/hr) and Consider IV bolus dose of 5000 units (see STEP 1) and if APTT ratio remains ≤1.5 despite this action, consult Haematology |
Recheck after 6hrs |
| 1.6-1.9 | ↑ by 200 units/hour ( = ↑ by 0.4 ml/ hour) and Consider IV bolus dose of 2500 units (see to STEP 1) |
Recheck after 6hrs |
| 2.0-2.5 | No Δ in infusion rate | Recheck after 6hrs |
| 2.6-3.0 | ↓ by 100 units/hr (= ↓ by 0.2ml/hr) | Recheck after 6hrs |
| 3.1-4.0 | Stop for 30 minutes. ↓ by 200 units/hr (= ↓ by 0.4ml/hr) | Recheck after 6hrs |
| 4.1-5.0 | Stop for 1 hour. ↓ by 300 units/hr (= ↓ by 0.6ml/hr) | Recheck after 6hrs |
| >5.0 | Stop for 1 hour and contact Haematology team ↓by 500 units/hr (=↓by 1ml/hr) |
Recheck after 2 hrs |
Bolus dose
Bolus dose for patients who have not received heparin within the last 6 hours.
Preparation: Heparin Sodium Injection 1,000 units/ml.
Dose: prescribe 5000 units as stat dose: 5mls of 1,000 units/ml. If bolus dose is not to be administered or was administered previously (e.g. Cath Lab), the prescriber should sign in the administration chart to signify this.
IV continuous infusion
We use Heparin 1,000 unit/ml in CUH. Please check your local policy.
In CUH, please:
- Draw up 25ml of Unfractionated Heparin 1000 units/ ml in a syringe (use five vials of 5000 units/ 5ml)
- Add 25mls of 0.9% sodium chloride to produce a concentration of 500 units/ml
- Administer via a syringe pump:
- Start the infusion at a rate of 2mls/hour (1,000 units/hour)
- Check APTT ratio/APTT (secs) 6 hours after infusion start
- Sampling: Do not take coag. samples from lines or from veins proximal to the site of the heparin infusion, as this may lead to erroneous results
Dosing for extremes of body weight
Dose adjustments to both the bolus dose and the initial infusion dose may be necessary at extremes of bodyweight (<50kg, >100kg). Please contact Consultant/Haematology in these cases.
Restarting after temporary break in infusion
If restarting infusion after a temporary break (e.g. procedure) restart at the rate that had achieved the target APTT as this is based on the individual patient’s response.
Administration chart
- A Heparin Infusion Prescription Chart is available to document prescribing and administration of variable dosing of heparin
- If using the Heparin Infusion Prescription Chart, prescribe on the regular section: ‘heparin infusion - see separate infusion chart’
Heparin induced thrombocytopenia (HIT)
- All patients who are to receive heparin should have a platelet count on the day of starting treatment
- For patients previously exposed to heparin in the last 100 days, obtain a platelet count 24 hours after starting heparin
- For all other patients, alternate day platelet counts should be performed from days 4 to 14 of therapy
- Signs of HIT include a 50% reduction of platelet count, thrombosis, or skin allergy
- If HIT is strongly suspected or confirmed, contact haematology
Links / References