Frostbite is the damage sustained by tissues while subject to temperatures below their freezing point (typically -0.5°C)
Can include non-freezing cold injuries (tissues not frozen but prolonged cooling)
Severity of frostbite injury is proportional to the temperature, duration of exposure, and amount and depth of frozen tissue
Note
Prevention is key
Rewarm frostbite as soon as risk of refreezing is minimal
Consider thrombolysis (tPA) in severe injuries presenting within 24 hours of exposure
Delay surgery unless evidence of compartment synd or overwhelming sepsis
Predisposing factors
General: Unusually cold weather, prolonged exposure to cold, inadequate clothing, inadequate use of appropriate clothing, homelessness, smoking, dehydration, old age, ethnic origin, high altitude
Most severe damage with freeze, thaw, and freeze again
Assess
Note details how injury occurred, likely temperature, wind chill, and duration of exposure—factors
Pre-morbid state (NB peripheral vascular disease, smoking, diabetes, medications)
Ascertain if injury occurred < (suitable for thrombolysis) or > 24 hours ago and decide if mild or severe
Clinical
Features of Frostbite
Early features
Late Features
Affected part feels cold ± painful
White and waxy skin with distinct demarcation
Continued freezing produces paraesthesia / numbness
Woody insensate tissues
Areas or blanching blending into areas of uninjured skin
Progression to bruising and blister formation (usually on thawing)
Degrees of frostbite
Clinical appearance
Mild frostbite injury
Severe frostbite injury
1st degree
2nd degree
3rd degree
4th degree
Depth of tissue freezing
Partial thickness skin freezing
Full thickness skin freezing
Freezing of the skin and subcutaneous tissue
Freezing of the skin, subcutaneous tissue, muscle, tendon, and bone
Colour of tissues
Erythematous or hyperaemic
Erythematous
Blue or black
Initially deep red and mottled; eventually black and mummified
Blistering or necrosis
None
Blistering (clear fluid)
haemorrhagic blistering an some tissue necrosis
Profound necrosis
Oedema
Minor
Substantial
Substantial
Little or none
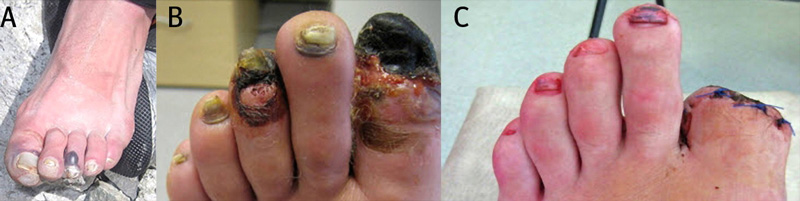
Fig 1 A typical frostbite affecting the hallux and third left toes showing the initial injury at presentation at base camp on Everest (A), at six weeks (B), and at 10 weeks (C). Note the delayed surgical amputation of the hallux after definitive demarcation and the recovery of the third digit after appropriate management