Aetiology
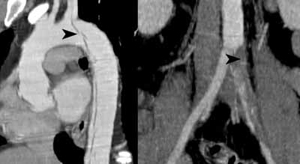
Dissection results from a tear in the aortic intima, which cleaves a plane in the media and allows blood to enter the false lumen. Arterial pressure extends the dissection for a variable distance distally and sometimes proximally.
- M:F = 3:1. Peak 50-70yo
- Mortality is about 1% per hour for the first 48 hours
- Aetiolog often unknown but associated with:
- Hypertension
- Marfan’s syndrome
- Ehlers-Danlos syndrome
- Aortic coarctation
- Aortitis
- Trauma
- Pregnancy
- Cocaine use
Presentation
- Chest pain (sudden onset, "ripping"). May also have myocardial ischaemia pain if involving coronaries. May radiate to back
- Painless in 10%
- Neurological symptoms (radicular pain / stroke), syncope, limb pain, dysphagia
- Symptoms of organ / limb ischaemia

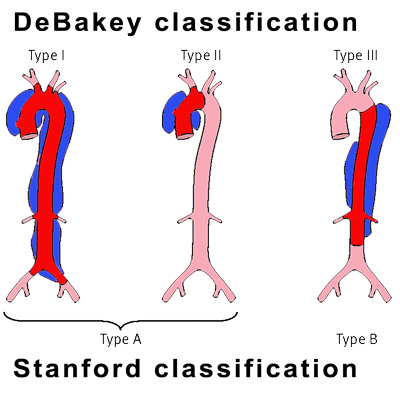
Classification
Stanford type A dissection
- Involves the ascending aorta
- 75% of all cases of dissection
- Presents with anterior chest pain
- Treatment = emergency cardiothoracic surgery
- Mortality 50% if no treatment
- Cardiac tamponade
- Aortic rupture
- AMI, aortic regurgitation if involves aortic root
Stanford type B dissection
- Starts distal to the left subclavian artery
- Presents with inter-scapular back pain (ripping)
- Divided clinically into uncomplicated and complicated (20%)
- Complications:
- Organ ischaemia (flap occluding vessel)
- Renal, splenic, mesenteric, spinal infarction
- Later aneurysmal dilatation of the aorta (20%
- Organ ischaemia (flap occluding vessel)
Treatment type A
- Surgery - open resection & replacement aortic segment
- Surgical mortality 30%
- High rate complications (organ/limb/spinal/brain ischaemia)
Treatment type B
- Uncomplicated dissections treated medically
- Control hypertension - analgesia, β block ±nitrates
- Complicated dissections require surgery
Summary of Systematic Review
A normal D-dimer excludes acute aortic dissection.[Eur Heart J. 2007 Dec;28(24):3067-75]. PMID: 17986466.
- 16 studies (437 patients), >D-dimer:
- High sensitivity (0.97 95% CI 0.94-0.98)
- High neg LR (0.06 95% CI 0.02-0.13)
- A negative D-dimer will exclude AAD