Background
- RNA virus
- Morbillivirus genus
- Paramyxoviridae family
- Highly contagious
- Respiratory transmission
- Winter and early spring
- Incubation period 7-10 days
- 2024: High incidence in parts of the UK/Eastern Europe (beware travel Hx)
Complications
Assoc. immunosuppress
- Otitis media
- Bronchopneumonia
- LTB (croup)
Coagulation
- Haemorrhagic measles
- Hepatitis
- DIC
Encephalitis
- 1:1000 get encephalitis
- These at risk of SSPE
Clinical suspicion
Consider the diagnosis of measles in all children (and adult) presenting with: fever, rash, cough, conjunctivitis
- Prodromal 3Cs
- Malaise, Conjunctivitis, Cough (tracheobronchitis), Coryza
- Initial fever (usually high) x4/7
- Koplik spots (salt grain or bluish by 2nd molar) day 5-7
- Rash day 7 (lasts 5 days)
- Starts on face ears, spreads centrifugally
- Maculopapular then confluent
- Involves palms and soles
- Generalised lymphadenopathy
- Hepatomegaly
- Abdo. pain (appendicitis or mesenteric adenitis)
- Cough often late (and last to resolve)
- Resolution by day 14


DDx
Rubella (German measles)
- Rubella virus (measles = rubeola paramyxovirus)
- Clinically almost identically
- Covered by MMR vaccine
- Rash and fever appear simultaneously in Rubella
- Rash similar distribution but finer and flat ±itchy
- Brownish/desquamation as rash resolves
- More dangerous to foetus (beware pregnant contacts/staff)
Approach, Mx and Ix similar to measles (rubeola).
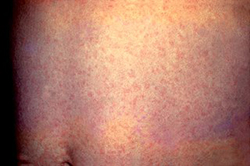
image from m.wikipedia.org/
Investigations in CUH
- Swabs available from Serology lab and stock kept in Controlled drug cupboard ED (advised 5 swabs in stock at all times)
- Remove blue swab from packet. Rub the blue swab along the gum line for time indicated on packet (currently 60 sec.)
- Place wet swab back inside the clear tube and replace the cap. Write patient's name, DOB and today's date on it- clear sample bag- check/ complete request form/order

Management
- Management is primarily supportive
- Vitamin A supplements
What to do if you have a suspected case:
- Isolate patient (plus infection control)
- An “oracol” oral fluid swab should be sent to the Micro. lab. Swabs are available in the treatment room CUH CED. Please record the date of rash onset and the vaccination history on the form when sending a swab
- In addition to the above PCR testing, Serum based testing for measles IgM, for serum collected 4 days after rash onset, and measles IgG are available 7 days a week in the NVRL
- Ensure staff are protected (MMR, previous exposure, born before 1978)
- Unimmunised children requiring admission should be immunised if no contraindications
- Opportunistic MMR immunisation is encouraged in other children who attend the ED
- Measles is a notifiable disease. If in the HSE South please inform on 066 7184548 of any suspect case as soon as possible. Outside of normal working hours the Public Health Doctor on call for emergencies can be contacted through the Ambulance Services at 021-4209848
- For those unfortunate enough not to live in Cork, here is a list of regional medical officer contact details
- Please complete a Measles - Surveillance form
Infection prevention and control measures
- If possible, assess the patient an a room which can remain vacant for two hours post consultation with suspected cases
- Suspected cases of measles should be placed in an airborne isolation room with controlled ventilation where possible
- Provide persons with signs or symptoms of measles with information on all infection prevention and control precautions
- Staff should use appropriate PPE (to include FFP2 mask) and standard and transmission based precautions
- Use standard and airborne precautions and contact with discharges from respiratory and mucous membranes with known or suspected measles
- Adhere to respiratory hygiene, cough etiquette and hand hygiene
- Adhere to environmental and equipment cleaning and disinfection
Links
- The posters and leaflets are located at https://www.hpsc.ie/A-Z/VaccinePreventable/Measles/Publications/
- HPSC guidance on measles
- List of regional medical officer contact details
- Measles - Surveillance form (please complete)
- HSE Measles patient information (May 2024)
- CUH Measles Pathway June 2025
- National Clinical Guidelines Infection Prevention and Control
- Point Of Care Risk Assessment (PCRA), Infection prevention & control (IPC)