Background
Remember analgesia (see analgesia section)
Always assess and record the patient's ability to bear weight
Hip fractures or dislocations
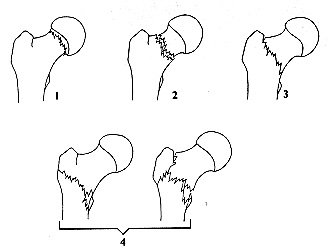
4. Inter or Sub trochanteric (Extracapsular)
AP and lateral X-rays required plus CXR if fractured. Check sciatic nerve and pulses. For fractures - complete fast-track documentation, add femoral nerve block to opiate analgesia. Admit under the on-call Orthopaedic Team.
Undisplaced fractures of the femoral neck
- May not be evident radiologically
- 1% of hip fractures will have a completely normal x-ray
- Patients may be able to walk with an undisplaced fracture
- In 5% of cases there may be no Hx of trauma (osteoporotic or pathological # likely)
Intracapsular (subcapital) fractures in young patients are an orthopaedic emergencies.
- Refer immediately to the duty orthopaedic SpR
- If inability to bear weight or significant pain on walking obtain an orthopaedic opinion
- For fractures of pubic rami, please see under 'pelvic fractures'
- In children beware of Perthes' disease (avascular necrosis aged 3 - 8) and slipped upper femoral epiphysis (occurring around puberty) which requires a lateral radiograph for diagnosis. Please see Hip Pain in Children
Femoral shaft fractures
- Check and treat ABCs
- Establish IV access and x-match 4 units
- Consider femoral nerve block
- Confirm distal perfusion and sicatic nerve function
- Apply Thomas or Donway traction splint worn until the patient goes to theatre