All suspected dislocations triage category 2 (document pain score and neurovascular status)
Always X-ray for fracture - except with a recurrent dislocation in a shoulder known to be unstable and which has occurred with minimal force
Reduction should be attempted first using Entonox, reassurance and a gentle manoeuvre
If this fails then manipulate after premedication with sedative and narcotic (NB follow sedation chart instructions) by an assisting doctor or arrange a GA, particularly in a muscular patient
Beware respiratory depression after narcotic and sedative and in frail individuals. Full resuscitation facilities must be immediately available
Always check x-ray and record neurovascular status after reduction
Sling (under clothes for under 40's, outside clothes in older patients) and refer to VFAC
Advise the shoulder will be immobilised for three weeks [Bestbets]
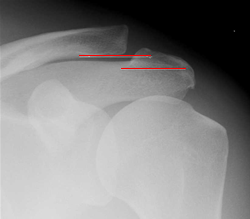
Posterior dislocation of the shoulder
Painful shoulder after direct anterior trauma or after epileptic fit or electrocution
May have surprisingly good range of movement (but painful ++)
Depression (rather than fullness of humeral head) below acromion
Absence of anterior dislocation on examination
Check neurovascular status
Internal rotation gives 'Light bulb' sign or overlap of glenoid and humeral head on PA view (right)